What is ASIT
The most important thing you should know when thinking about treating allergies is that with the help of ASIT you can only fight a reaction to the major (major) proteins of the allergen.
You can find out which proteins, major or minor, the allergic person’s body reacts to based on the results of an analysis for allergic components using the ImmunoCup method or AllergoChip, Allergo Expert 300 and ALEX analysis.
These tests are very important for predicting the outcome of ASIT and for the competent selection of ASIT itself.
Next, let's move on to the theory.
Allergen-specific immunotherapy or ASIT is the only method for treating respiratory allergies today, which has been used for more than 100 years.
The effectiveness of ASIT is confirmed by research from the World Health Organization (WHO).
Immunotherapy is needed to dull the body's response to the allergen. To do this, gradually increasing doses of the allergen are introduced into the allergy sufferer's body.
The reaction of the immune system of an allergic person changes under the influence of micro doses of the allergen and, as a result, its susceptibility to this allergen is significantly reduced.
This is to put it quite simply.
For those who are forced by allergies to study chemistry, I’ll explain it a little differently.
During ASIT, the immune system receives small but constant doses of the allergen, which reduces the level of E-immunoglobulins (IgE), responsible for the allergic reaction.
Instead of immunoglobulin IgE, ASIT activates the production of G-immunoglobulin IgG4, which blocks the allergic reaction. The IgG4 indicator is the only laboratory test that determines the functioning of ASIT. Ideally, the level of specific immunoglobulin IgE should decrease, and the level of IgG4 should increase. However, the allergist's main conclusions are based on the patient's symptoms.
In Russia, an IgG4 test, unfortunately, is rarely prescribed. Russian allergists monitor the progress of therapy using the patient’s diary.
The total duration of therapy is from 3 to 6 years.
Indications for ASIT therapy
ASIT is prescribed when there is a history of IgE-dependent confirmed allergic diseases. Treatment is carried out using exclusively standardized medications, the safety and effectiveness of which have been proven in practice.
An allergist-immunologist prescribes ASIT if there is a history of confirmed IgE-dependent allergic diseases. Treatment is carried out using standardized drugs, the effectiveness and safety of which have been proven in practice.
Why is ASIT needed?
Currently, ASIT is the only way to treat allergies that not only relieves symptoms, but also gets rid of the causes of allergies.
The main goal of ASIT is to reduce the number of medications that an allergic person takes.
Immunotherapy can put allergies into remission, that is, reduce the manifestations of the disease, until symptoms disappear completely.
It is important to know that the earlier ASIT is started, after the first manifestations of allergies, the longer the remission. Remission can last up to 20 years, and 5% of allergy sufferers forget about allergies forever after ASIT.
ASIT can also be a preventative method for allergies to other allergens.
Immunotherapy interrupts the growth of allergies and prevents mild allergic reactions from developing into more serious ones, such as bronchial asthma, Quincke's edema or anaphylactic shock.
With a competent approach from the doctor and the responsibility of the patient, the positive effect of ASIT is achieved in 95% of children from 5 to 11 years old, in 80% of adolescents from 11 to 14 years old, and in 70% of people over 14 years old.
Benefits of specific hyposensitization
After a course of specific therapy, in 9 out of 10 patients with diagnosed allergic rhinitis or hay fever, the elimination of individual allergic symptoms, a decrease in their severity, or complete recovery was noted. The result of this treatment was a reduction in the need to take medications, as well as the transition of allergies to a low degree of activity.
With the help of ASIT therapy, you can significantly reduce or completely eliminate symptoms for quite a long time, as well as significantly delay the period of remission. After this course, the need to take symptomatic anti-allergy drugs is significantly reduced.
Allergy vaccination is the best way to prevent the expansion of the spectrum of allergens. It also prevents the transition of rhinitis to bronchial asthma.
Types of immunotherapy
There are several main methods of therapy. At the consultation, the allergist, having studied our history, recommended drops under the tongue for my son. We didn’t even consider injections because of the baby’s panicky fear of needles.
The most popular types of ASIT in our country:
- Injection (injections);
- Sublingual (drops under the tongue and tablets).
The effectiveness of the sublingual and injection methods is equivalent.
Sublingual ASIT depends on the total dose collected and is not recommended if the oral mucosa of an allergic person reacts to many food crossovers.
The injection method has a greater number of side effects, including serious ones.
Features of sublingual immunotherapy (SLIT):
- painless;
- carried out independently at home;
- a visit to an allergist is required when taking the drug for the first time and to monitor treatment;
- the likelihood of severe reactions is almost zero;
- requires daily use (see instructions);
- a variety of dosage options (from the ability to split the medication into several doses to spitting out the drug).
Possible side effects of SLIT:
- sore throat;
- itching in the mouth;
- swelling in the sublingual area, which does not interfere with swallowing;
- ear itching;
- sneezing;
- cough;
- the appearance of nasal congestion;
- exacerbation of atopy (my child first developed atopy against the background of ASIT);
- diarrhea;
- headache;
- nausea and vomiting.
If reactions occur and go away on their own within the first 30 minutes after using the medicine, no additional treatment is needed. If adverse reactions recur several times in a row, stop ASIT and contact an allergist to clarify further actions.
Features of injection immunotherapy (iASIT)
- carried out only by an allergist in a specialized institution where it is possible to provide emergency care;
- It is prohibited to conduct it at home;
- injections may be painful;
- dosage regimen at the dose set stage - once a week, at the maintenance stage - once a month (the allergist may prescribe a different regimen);
- high risk of severe allergic reactions.
Possible adverse reactions to ASIT:
- redness and swelling at the injection site;
- the appearance of nasal congestion;
- headache;
- nausea;
- weakness;
- cough;
- itching;
- attack of bronchial asthma.
Reactions can occur within a period of half an hour to several hours, or the next day. The attending physician should be aware of all adverse reactions without exception.
Main comparative characteristics of sublingual and subcutaneous ASIT
| Characteristics | Sublingual ASIT | Subcutaneous ASIT |
| Efficiency | High effectiveness confirmed based on meta-analysis | High effectiveness confirmed based on meta-analysis |
| Safety | Most secure | There is a risk of developing systemic reactions |
| Patient profile | Recommended for patients intolerant to ASIT, children due to fear of injections, patients who are unable to regularly visit a doctor for injections | Recommended for patients who need closer and more regular contact with their doctor |
| Concentration | High concentration of allergen | Reduced allergen concentration |
| Ease of use | Does not require the presence of medical personnel and can significantly save time for both the doctor and the patient | Requires the presence of medical personnel and more significant time expenditure for both the patient and the doctor |
Types of allergies that are treated with ASIT
My little allergy sufferer has a reaction to birch, cat and dust. As our allergist says, we are classic allergy sufferers. Three years ago in St. Petersburg they had not yet done ASIT for cat hair. Now the situation has changed for the better. Although immunotherapy against animal fur is still not officially approved in Russia, many allergists carry it out with imported drugs.
Today, Russian allergists use ASIT to treat the following types of allergies:
- allergy to pollen of the birch family;
- for weeds - wormwood and ragweed (in 2020, the Danish drug Ragvisax was certified in Russia);
- on meadow grasses;
- for house dust mites;
- allergies to pet hair and mold (in Russia, drugs for ASIT for animal hair and mold are still not certified, but many allergists still carry out immunotherapy for these allergens, mainly using Spanish and German drugs);
- for poisons of stinging insects (the drugs are not officially certified, but you can find them).
Around the world, immunotherapy is used to combat allergies:
- to the poisons of stinging insects;
- for mold;
- for pollen of the birch family;
- on weeds and wormwood;
- on meadow grasses;
- for house dust mites;
- on pet hair.
Allergies, modern methods of diagnosis and treatment
How to make your life easier with allergies? Is it inherited? What new treatments have emerged? These and other questions are answered by the chief freelance specialist - allergist-immunologist of the capital's Department of Health, Alexander Pampura.
Spring has finally broken through to the capital, and soon most Muscovites will enjoy the greenery, warmth and sun. Unfortunately, many will instead start sneezing, coughing and crying due to pollen allergies. Is it possible to get rid of the spring scourge, what manifestations of allergies are the most dangerous and what is the hygienic theory - in the material Mos.ru.
— Alexander Nikolaevich, what are the main symptoms of allergies?
— Symptoms depend on the individual and are largely related to the type of allergy. For example, if there is hypersensitivity to food products, then these are primarily skin manifestations and damage to the gastrointestinal tract. If you are allergic to inhaled irritants—pollen and animal dander—then you may experience sneezing, coughing, and difficulty breathing.
— What time of year is the peak of allergies? Spring?
- On our territory - yes, April - May. People who are sensitive to birch, alder and hazel pollen suffer. They should try to avoid allergens: go out less in sunny, windy weather, and go around parks and squares. You also need to wear a cap or headscarf and sunglasses. Medical masks do not help; moreover, allergens can accumulate on them and it will only get worse. You must turn on the air conditioning in the car and keep the windows open. Same thing at home.
— Is it possible to prepare in advance to make your life easier in the spring?
— The modern method of treatment is allergen-specific immunotherapy. Its meaning is that the patient is first given small doses of the allergen, and then gradually increased. And after some time the person simply stops responding to the stimulus. But with this method, the patient’s motivation, good contact with the doctor and willingness to follow all his recommendations are very important. In addition, this is a long-term therapy: the effect is usually assessed in the second or third year of treatment.
— Is this therapy carried out throughout the year?
— There are several treatment regimens. The most common are injection and sublingual (under the tongue - approx. mos.ru)
introduction of allergens. Typically, allergen-specific immunotherapy begins several months before flowering and a certain number of injections are given. The procedure is repeated the following year. By the way, this can be used to treat allergies not only to pollen, but also to house dust mites.
— Is it necessary to treat pollen allergies at all? Or is it easier to wait a couple of months a year?
— It is necessary to treat, because allergies greatly impair the quality of life. For example, seasonal rhinitis reduces students' academic performance by an average of one point.
The most dangerous nosology is anaphylactic reaction. It can occur to different allergens. But most often - for food or medicine
— What type of allergy is the most dangerous and can lead to death?
— The most dangerous nosology is anaphylactic reaction. It can occur to different allergens. But most often - for food or medicine. Anaphylaxis causes symptoms from at least two body systems. For example, rashes appear on the skin and at the same time it becomes difficult to breathe.
- How many people suffer from such hypersensitivity?
— About two percent of the population, this is a big figure and a huge problem for the whole world. Children most often react to milk, eggs, and fish. Adults eat peanuts and seafood. Even in adults, especially the elderly, a severe reaction to medications is added. First of all, on antibacterial drugs and local anesthetics. Anaphylaxis can also occur during operations when a large number of drugs are administered to a person. The extreme manifestation of anaphylaxis is anaphylactic shock.
- But people suffering from such a severe form know about their allergies?
— When this happens for the first time, as a rule, they don’t know.
— What should others do if a person develops anaphylaxis?
- In general, you need to use adrenaline. But usually no one carries it with them, so you need to call an ambulance. After the first episode, it is very important that the person consult a specialist and be diagnosed with anaphylaxis. Because next time the attack may be more severe. After the patient has been diagnosed, he receives a special package with the necessary medications and a description of the sequence of actions.
— There is a theory on the Internet that allergies are treated through anaphylactic shock.
- This is extremism, adequate specialists do not deal with this.
— Can a person find out in advance whether he is allergic to pets?
— Yes, you can conduct a diagnosis before getting a pet. But there are situations when the test shows a negative result, people get an animal, and after some time the allergy still manifests itself. Moreover, this can happen even after a few years.
— Some doctors advise girls to remove pets during pregnancy so that the child does not develop allergies. Others are the opposite. Who to believe?
- If there were animals in the house, then there is no need to get rid of them during pregnancy. We advise expectant mothers the following: do not smoke, avoid stress, do not take antibiotics unless necessary. And it is also important not to narrow your diet, that is, to eat as usual.
— What are some tips for preventing allergic diseases in children?
— What we just talked about is prevention. And after the birth of a child, breastfeeding is necessary for at least three to four months. Again, no smoking. It is also recommended to moisturize the baby’s skin. This primarily applies to children with a predisposition, that is, those whose closest relatives are allergic.
— What types of allergies are inherited?
— It is not the disease that is inherited, but the predisposition to it. For example, if both mom and dad have allergies, there is a 70 to 80 percent chance that the baby will have them too. But the number of children with hereditary complications is only 30–40 percent of all allergy sufferers. That is, healthy parents can have a child with allergies and, conversely, allergy sufferers can have a healthy child. Therefore, it is currently impossible to create a universal prevention program for all children. This is a big problem.
— What diseases can be hidden behind the symptoms of hypersensitivity?
— First of all, ARVI. Therefore, in the spring, when the trees are blooming, many people think that they have an allergy, but in fact it is a respiratory infection. It is better to consult a doctor and clarify the situation.
— Where in the capital can you get tested to understand what exactly you are allergic to?
— Many city hospitals and clinics have allergists. There is also a specialized center for allergy and immunology in the city clinical hospital No. 52.
— What types of allergies do Muscovites most often turn to doctors for and what is the reason for this?
— The appeal is related to the season. Due to the high exposure to pollen allergens, people mostly come with allergic rhinitis and bronchial obstruction in the spring. In winter, people often turn to us because of symptoms of bronchial asthma: people spend a lot of time in closed, heated rooms, and under these conditions, house dust mites are activated.
— How many allergy sufferers are there in Moscow?
— Large-scale epidemiological studies have not been carried out in Moscow. But we can focus on European figures: at least 20–30 percent of the population suffers from allergic diseases.
— Can we base it on the number of people who went to the doctor?
— This will be the turnover, and not general statistics. A striking example is allergic rhinitis, which affects at least 15 percent of the population. And those who turned to a specialist are only three to five percent.
— Let’s say a person comes to the doctor and wants to find out what he is allergic to. How is the research conducted?
— Allergy diagnostics begins with collecting information about the patient. Next, the most optimal tests for a particular patient are selected and research is carried out with the most common allergens. These include, for example, eggs, milk, fish and wheat.
Currently, we have the opportunity to carry out molecular diagnostics using allergy chips. They simultaneously test for 112 allergens, including sensitivity to specific proteins. Thanks to this, we know which protein the patient reacts to. Accordingly, we understand how severe his reactions may be and what methods are best to treat him.
- What medications?
— Medicines, including, but not only. In fact, the main thing is personalization of therapy, an individual approach. If a patient leaves the doctor with a huge list of things to exclude, the consultation will most likely be ineffective. You need to dig deeper: look not only at the test results, but also at the medical history, analyze the patient’s complaints and objective data. It is necessary to find out what exactly the allergy is to and make targeted exceptions so that the person’s lifestyle changes minimally. Figuratively speaking, do not try to put an allergy sufferer in a glass cabinet. Plus, the doctor must foresee how the disease will progress and prevent possible problems. The most recent research and treatment methods involve so-called targeted therapy. Monoclonal antibodies are selected for a molecule that is significant for the patient. This is a fashionable therapy, it is now actively developing. Perhaps this will be a breakthrough in allergology. But as you understand, the drugs are completely new, so treatment will be very expensive.
— Is it already being used somewhere or is it still undergoing clinical trials?
— Some drugs are already being used. Others are about to appear: they are undergoing phases three or four of clinical trials.
Another direction is, let’s say, a new round of allergen-specific immunotherapy, which we have already talked about. The patient is injected not just with an allergen, but with a specific protein to which there is a reaction. Efficiency increases significantly.
— You were one of the initiators of the formation of a register of patients with severe allergic reactions. What is it and why is it needed?
— The register includes the patient’s passport data, symptoms, diagnosis, changes that occur, response to therapy, and so on. I would like to note that everything is confidential and only doctors can have access to this information. It is very important to create a registry of patients with severe reactions, in particular anaphylactic ones. This will give an idea of the real situation with allergic diseases. It will be easier for doctors to identify risk factors, monitor diseases, and prescribe the correct treatment. The register will help systematize knowledge and share experience.
All developed European countries already have this. Moreover, there are national registers, regional and city registers.
— At what stage is the Moscow one now?
— A working version already exists, patients are being accumulated.
— Patients with what diagnoses will be included?
- Anaphylaxis, Lyell's syndrome, Stevens-Johnson syndrome, severe chronic urticaria.
— The number of allergy sufferers is increasing every year. Many experts attribute this to improved hygiene. Do you agree with them?
— The prevalence of allergic diseases in the 1960s was two to three percent of the population. Now in developed countries there are already 40–50 percent of allergy sufferers. It is clear that this is not related to genetics, because it could not change in just 50–60 years. A lot of hypotheses have been put forward, and in particular the “hygienic” one. In a simplified form, it sounds like this: the cleaner it is, the greater the likelihood of developing an allergy.
Firstly, due to the decrease in the number of infections, the activation of our immune system has decreased and we have become more likely to suffer from allergic diseases. There is a balance between the response to the allergen and the response to the infection. And infections have decreased thanks to vaccination. But we must understand that the potential risk of developing allergies is incomparable to the benefits of vaccination. Secondly, a huge amount of detergents appeared, and thirdly, the diet changed fundamentally.
Of course, the “hygienic” theory has a right to exist. But it should be approached from a scientific perspective. Don't eat with dirty hands, walk unwashed and be afraid of detergents - this is wrong. We, after all, are civilized people and live in a metropolis. You must maintain hygiene and try to maintain a healthy lifestyle.
Link to material: https://www.mos.ru/news/item/22941073/
What drugs are used for ASIT?
When we decided on therapy, we had to choose the drug that would be used for ASIT. Our main allergen is birch, and for a long time I chose between the Spanish medicines Diater and the French Staloral. The decision was not easy. Spanish drugs are considered one of the best in the treatment of allergies, but I had to choose French ones, as they are easier to buy in our pharmacies.
Typically, allergens that comply with the AU (Allergу units) standard developed in the USA and the European BU (Biological units) standard are used for immunotherapy.
Spanish, French, Italian, German and Danish are considered high-quality drugs for ASIT.
Russian and Czech drugs are less purified and of poorer quality.
In Russia, French, Italian, Danish and Czech medicines for ASIT are certified.
It seems that certification of Spanish drugs in our country is not far off, since, according to rumors, a plant is being built in Moscow where they will produce medicines for allergy sufferers using Spanish technologies.
There are several forms of drugs for ACIT
Water-salt extracts
For the most part, these are medicines from Russian manufacturers. For example, the NPO MicroGen company produces injectable preparations of oak, birch pollen and other allergens.
The same group includes Kazakh medicines “ Antipollin ” for allergies to pollen from weeds and meadows, wormwood, trees and house dust. “Antipollin” is registered as a dietary supplement.
Allergoids
Allergoids are chemically transformed allergens with low allergenic activity that cause a less severe reaction and reduce the likelihood of side effects. Allergoids enhance the body's immune response. ASIT can be performed simultaneously with two types of allergoids as effectively as with one.
Each drug comes with instructions, but the treatment regimen and minimum doses must be determined by an allergist.
Most imported drugs for ASIT are allergoids.
Danish ALK campaign drugs
Three sublingual drugs have been certified in Russia:
- Acarizax is a house dust mite allergen (allowed from 12 years of age).
- Ragvisax is an allergen of ragweed (allowed from 18 years of age).
- Grazax - an allergen of grass pollen (timothy grass) - allowed from 5 years.
Soon they promise to certify the birch allergen. All three drugs are available in tablet form, which taste pleasant and dissolve quickly in the mouth. Shelf life: 5 years. No need to store in the refrigerator.

Preparations of the French Stallergenes campaign
Stallergenes produces a large number of different vaccines. Certified in Russia:
- Allergens Staloral and Oralair for sublingual ACIT;
- Alustal and Fostal for subcutaneous ACIT (Fostal is temporarily not on sale due to equipment modernization).
Italian Lofarma
Lofarma preparations are certified in Russia.
German Allergopharma
Not certified in Russia, but you can find allergists who work with these drugs. Allergopharma produces both injections and preparations for sublingual ASIT. Allowed for use from 5 years of age.
Spanish: ImmunoTek (Alxoid, Oraltek), Diater
The drugs are popular all over the world, but are not yet certified in Russia.
There is a detailed article on the website about Spanish drugs.
Who is prescribed ASIT?
Treatment is prescribed and carried out by an allergist.
Immunotherapy is not prescribed to all allergy sufferers. Firstly, to prescribe ASIT, an allergy sufferer must have recurring and worsening respiratory allergy symptoms from season to season. For example, ASIT may be prescribed to a child or adult with allergic rhinitis and cough, which may develop into mild or moderate asthma.
Secondly, the allergy sufferer must have a confirmed reaction to major proteins - inhaled (non-food) allergens. Because with the help of ASIT it is possible to cure a reaction only to major proteins. ASIT does not treat a reaction only to minor proteins of the allergen.
In our country, immunotherapy is usually prescribed to children from 5 years of age. But many Russian allergists, like their European colleagues, can prescribe ASIT from 4 or 3 years of age if they see that the allergy is rapidly progressing.
Diagnostics
THE INSTITUTE OF ALLERGOLOGY AND CLINICAL IMMUNOLOGY has a fundamental base that allows it to carry out the full range of diagnostic and therapeutic measures for any form of allergy that meets the level of international standards. Many of the diagnostic and treatment methods were developed by the staff of our Institute.
To establish a diagnosis, it is necessary to conduct examinations with the participation of specialists in various fields: an allergist-immunologist, a dermatovenerologist and doctors of other specialties. The diagnosis is established on the basis of the clinical picture, careful collection of anamnestic data, the establishment of hereditary predisposition, and a special allergological examination is performed.
LABORATORY DIAGNOSTICS:
The examination method and methodology should be determined by an allergist-immunologist!
Laboratory diagnostics for metals, plastics, liquid solutions
1. Consultation with an allergist-immunologist
2. Test for the risk of developing an anaphylactic reaction (determining the level of serum tryptase and histamine)
3. For different consistencies of drugs and substances, a decision is made to conduct diagnostics:
| In vivo (provocative tests) | In vitro |
| – Application test (patch test) – “Rinse test” | – Determination of allergen-specific IgE antibodies by ELISA – Determination of allergen-specific IgG antibodies by ELISA – Determination of total IgE by ELISA |
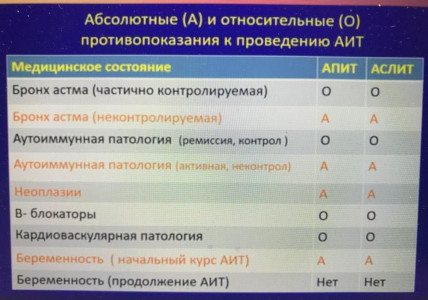
Contraindications
Immunotherapy is not prescribed:
- Allergy sufferers with a reaction only to minor proteins;
- If there were severe allergic reactions to the previous course of ASIT;
- For atopic dermatitis without respiratory manifestations to an allergen;
- For food allergies (for example, to fish. This type of immunotherapy is still at the research stage)
- People with autoimmune diseases (except for compensated thyroid diseases and type 1 diabetes);
- ASIT will be ineffective in case of immunodeficiency;
- Therapy is not prescribed for allergic diseases in the acute stage (temporary contraindication);
- Temporary contraindications for uncontrolled asthma;
- Allergy sufferers with cardiovascular diseases (it is impossible to safely use adrenaline);
- Patients with active tuberculosis and rheumatism;
- In case of impaired renal and liver function, hepatitis, nephritis;
- For blood diseases;
- Patients with mental disorders;
- Until 2020, ASIT was contraindicated in patients over 55 years of age. Currently there is no age limit;
- Allergy sufferers with cancer.
ASIT cannot be combined with treatment with adrenergic blockers (Atenolol, Lokren, Vasocardin and others).
ASIT cannot be combined with taking certain antidepressants (Isocarboxazid, Befol, Phenelzine and others).
What tests to take before immunotherapy
A list of tests should be prescribed by an allergist.
For more information about tests before ASIT, read the article: Analyzes before ASIT.
Here I will simply list a list of tests, without details of why they are prescribed.
- Analysis for minor and major proteins of the allergen (if you have a polyvalent allergy, then it is advisable to take a complete AllergoChip / Allergo Expert 300 / ALEX analysis);
- thyroid hormones (ultrasound);
- detailed clinical blood test;
- biochemical blood test (total protein, total bilirubin, glucose, ALT, AST, LDH);
- before ASIT injections: blood test for infections - syphilis, HIV, hepatitis B and C;
- general urine analysis;
- check the liver and pancreas;
- Vitamin D;
- ECG;
- FVD (as prescribed);
- endoscopic examination and consultation with an ENT doctor (if you have a year-round runny nose);
- Ultrasound.
How and when to start therapy
Before starting therapy, we completely had to change our usual life. With tears, we parted with the cat, threw out carpets and other dust collectors, took out flowers, gave the neighbors an aquarium, installed Tiona in all rooms and purified the air. All this is in order to stabilize the child’s condition.
ASIT is started in remission of an allergic disease. An allergy sufferer must have good nasal breathing (if there are nasal polyps, then ASIT is allowed with them). The allergy sufferer should not have asthma attacks (asthma control should be achieved).
If the problem with the nose cannot be solved, the doctor may decide to start immunotherapy for the “snotty” nose.
The effectiveness of sublingual ASIT will depend on the total volume of medication administered during one continuous course of therapy. Therefore, it is important to reduce the risk of any unstable conditions that may affect continuity of medication.
It is difficult to track a comfortable dose of the drug if an allergy sufferer has an exacerbation of any chronic diseases, since the body in this state can react acutely to the smallest amount of allergen.
When to start immunotherapy depends on the type of allergy. ASIT for pollen allergens - autumn, winter. For year-round allergens (house dust, animals, etc.) - all year round (if there are no contraindications).
If ASIT is carried out with injections, then you need to follow a diet. With the sublingual method, a diet is not needed (if there is no reaction).
Treatment of allergic rhinitis and bronchial asthma
Having suspected these diseases in yourself or your child, you turned to an allergist, confirmed the diagnosis and are now planning to undergo treatment. What exactly can we expect from therapy?
Treatment of respiratory allergies occurs in three directions:
- avoiding contact with the allergen (the most effective way),
- selection of drug therapy to combat symptoms and prevent them (such treatment is necessary so that unpleasant symptoms do not occur during the period of contact),
- allergen-specific therapy (treatment aimed at “accustoming” the body to the allergen).
Avoiding contact with the allergen remains the most effective way to get rid of allergy symptoms. If it is impossible to avoid contact (with hay fever, with dust allergies), rinsing the nose with an isotonic solution of sea salt or sodium chloride and using barrier sprays will be effective.
The fact is that the attachment of allergens to the nasal mucosa is a necessary condition for triggering an allergic reaction. If the allergen molecule fails to adhere to the mucous membrane, the reaction will not start, allergic inflammation will not occur, and the signs of allergy will decrease.1
Drug therapy in allergology in most cases is stepwise. The doctor selects it depending on the severity of the condition, and then can intensify it as needed. After achieving a stable condition, in some cases the doctor may gradually reduce the intensity of treatment (for example, when it comes to bronchial asthma).
The natural progression of allergies can lead to an increase in symptoms and the need for medication. In this case, the previously selected treatment may not be sufficient, and the person may mistakenly conclude that he is accustomed to the medicine. However, if the usual medications stop working , this may mean that the manifestations of allergic rhinitis or bronchial asthma have intensified and it is necessary to increase therapy.
Schemes for conducting ASIT
ASIT treatment regimens are not universal - they are unique for each method and drug and are selected individually by the allergist.
Classic scheme
Immunotherapy according to the classical scheme is carried out with a gradual increase and maintenance of a comfortable dosage over a period of 6 to 10 months without a break.
The total treatment period lasts from 3 to 6 years.
Treatment according to the classical scheme rarely produces side effects or complications, so there is no need for round-the-clock medical supervision.
If the drug is taken by the sublingual method, the treatment takes place at home. Injections are given at the clinic.
Short-term scheme
Short-term ACIT is carried out only in a hospital where it is possible to provide quick, qualified assistance. All methods of the short-term ASIT regimen are combined with the use of antihistamines.
Accelerated scheme
Injections of a solution with an allergen 2-3 times a day;
Lightning
Rush is a method.
The required dose of the allergen is administered subcutaneously three days in advance, every three hours in equal parts with adrenaline.
Shock method
Injections of a solution with an allergen and adrenaline are made every two hours during the day.
During ASIT against the venom of stinging insects, when therapy coincides with the time of their activity, it is advisable to constantly take antihistamines and observe precautions against bites.
Each scheme, with the exception of the shock method, is carried out in two stages.
The first stage begins with the introduction of a small dose of the drug, which is gradually increased to an optimally tolerated dose.
At the second stage, it is optimal - a tolerable amount of medication is administered regularly until the end of the ASIT course.
The dosage depends on the type and strength of the allergen, the method of administration and the individual reaction of the allergy sufferer.
How is ASIT performed?
Preparation
The decision on the advisability of specific immunotherapy is made jointly by the patient and the doctor. Before starting treatment, a person suffering from allergies will have to undergo training, which involves conducting research - their results are necessary to draw up an individual treatment regimen.
Mandatory examinations include blood and urine tests, as well as allergy tests. Additionally, the doctor may order an electrocardiogram and spirography (the list of necessary examinations depends on the characteristics of the disease and the patient’s condition).
A week before the procedure, the patient should stop taking antihistamines. During the treatment course, it is important to create such conditions to avoid contact with the provoking allergen (or at least reduce it to a minimum).
Options
Allergen immunotherapy can be performed on an outpatient or inpatient basis. In the first case, one treatment course lasts up to six months (such courses are repeated for several years in a row). If the patient is in a hospital, vaccination is carried out for 3–4 weeks, after which another 2–3 months of procedures are carried out on an outpatient basis.
Scheme
There are several schemes of hyposensitizing therapy. The best option is the classic scheme, which is suitable for various forms of allergies - both at an early stage and with a long-term illness. As an alternative, the patient may be offered a shortened version that takes less time. Accelerated courses carry more risks, so they can only be carried out in mild forms and in a hospital setting, under constant medical supervision.
Without exception, all schemes consist of two stages:
- At the first stage, the introduction of minimal doses of allergens begins with their gradual increase to the maximum permissible dose (this is the so-called optimal dose, the maximum tolerated volume of the allergen). In the classic version, this stage, called the initiating stage, usually lasts 4 months.
- The second stage is the maintenance stage (according to the classical scheme, it lasts from 6 months to several years). All this time, the patient receives an optimal dose of purified allergen - this allows the achieved effect to be consolidated.
Methods of administration
To deliver the allergen into the body, ASIT therapy provides injection and non-injection methods of administration:
- Using subcutaneous injections (shots);
- orally (in the form of tablets, drops, capsules);
- sublingual (absorption under the tongue);
- intranasally (instillation into the nose).
The most convenient and safest method is sublingual administration, which can be used in both adult patients and children.

Figure 4 - Subcutaneous injection
ASIT treatment - drugs
The patient may be offered different forms of drugs. Initially, therapy using this method involved the use of water-salt extracts (for example, a water-salt preparation of birch pollen).
Later, in addition to natural allergens found in nature, modified polymerized analogs appeared - allergoids for injection and resorption.
In the arsenal of domestic allergists there are drugs of Russian and imported origin (medicinal allergens Stallerzhen, Alustal, Oralair, Staloral, etc. have proven themselves well).
Figure 5 — Allergen-specific immunotherapy
The most effective and safest are depot preparations (long-acting allergy vaccines). Their peculiarity is that the release of the allergen occurs directly in the body (this reduces the risk of side effects), and the effect of the drug lasts for a longer time, due to which fewer procedures are needed.
When is immunotherapy interrupted?
ASIT needs to be suspended:
- at high temperature;
- during vaccination (more details below);
- with severe reactions to treatment;
- with exacerbation of bronchial asthma.
ASIT, which is performed using the sublingual method, can be interrupted in the following cases:
- if there are wounds in the oral cavity (periodontitis, gingivitis, stomatitis);
- if a tooth falls out or is removed (we wait until the wound heals).
When my child’s baby teeth were loose, the doctor allowed ASIT to be performed until they fell out. If the break in therapy is less than 7 days, then you can continue taking the medications according to the previous regimen (what dosage you stopped at is where you start). If the break is more than one week, then the dosage should be discussed with your doctor.
ASIT can be resumed only with the consent and under the supervision of an allergist
Contraindications for the sublingual method of drug administration for ASIT
- · erosions, ulcers and other persistent damage to the oral mucosa;
- · persistent periodontal diseases;
- · recent surgical manipulations in the oral cavity;
- · gingivitis with characteristic bleeding gums;
- · diseases of the oral mucosa that are inflammatory in nature.
When a patient is diagnosed with hypersensitivity to several allergens at once, a mixture of allergens is used, but in this case, ASIT does not guarantee quick treatment results. To enhance the effect, immunomodulatory treatment is additionally carried out.
ACIT and vaccination
Before vaccination, be sure to tell your doctor that you are planning or undergoing ASIT.
The doctor will find a solution on how best to proceed depending on the situation. For example, if you are just planning to start ACIT, then the vaccination can be done at least a month before the start of the course of treatment.
If the time of vaccination coincides with the maximum dose of medication for ASIT, then you should refrain from vaccination.
The vaccination can be done during the maintenance course of ASIT, but provided that immunotherapy has been carried out without interruption for three or more years.
When ASIT is carried out using the sublingual method, the drug is stopped 3 days before vaccination, and treatment is resumed 2 weeks after vaccination.
For ASIT using the injection method, the regimen is determined by an allergist in each individual case.
It is not recommended to vaccinate and take the drug for ASIT on the same day.
What are the rules for allergen-specific immunotherapy?
We use several methods of ASIT: injection, oral, sublingual (the last two options mean that patients receive the drug in the form of tablets or sublingual drops). To begin any type of treatment using the ASIT method, it is necessary to identify an allergen or group of allergens leading to the development of symptoms of the disease. Allergy diagnostics are covered separately.
For injection immunotherapy, prepared allergens are used. For example, Fostal, Alustal, which are administered mainly intramuscularly. Our doctors follow all the new products and discoveries in the world and immediately try to introduce the best of them into their practical work.
ASIT for children

Immunotherapy usually starts at age 5. The safety of ASIT for younger children has not been studied. Our allergist was not against starting immunotherapy, on her own responsibility, for my son at the age of 4, since the child is at risk for developing asthma. But the child’s allergy began at the age of 3, and prescribing ASIT requires two seasons of observation, so therapy was postponed until 5 years.
The doctor immediately warned me that for stable remission, the duration of therapy should be at least 3-6 years, as in adults.
Children are more often treated with ASIT using the sublingual method. Since sublingual drops or tablets are convenient to use and they are safer. In addition, this method, unlike injections, traumatizes the child’s psyche much less.
During ASIT, parents should have constant contact with the attending physician to clarify any questions. And there will be questions, I have no doubt about that.